
By Linda Duckworth, CHC, CPC
Director, Provider Education & Advisory Services
One of the benefits of an Electronic Health Record (EHR) for Hospital Medicine is the ability to get us to where we are going quickly by bringing forward (copying and pasting) text, eliminating the need to recreate information from visit to visit. However, proceed with caution as this shortcut pearl has many hidden perils.
An enlightening article written by a group of physicians in JAMA, September 26, 2022, Prevalence and Sources of Duplicate Information in the Electronic Medical Record, spoke directly to quality and efficiency concerns with copy and paste, stating that cloning records makes it difficult to find relevant information when treating patients. According to the article,
Information overload and duplication are severe hazards for practicing clinicians. Finding the right information is no longer a matter of flipping through a paper chart; it is more akin to reading large portions of a book… Our analysis shows that roughly half of text is directly duplicated, word for word, from elsewhere in the record, compounding the challenge of finding the right data to make appropriate clinical decisions.
The authors warn, “Duplicated text is a well-documented hazard in electronic medical records (EMRs), leading to wasted clinician time, medical error, and burnout.”
The Centers for Medicare and Medicaid (CMS) (Medicare) are not fans of cloned records either, as they are continually pained by the perils of overbilling. In their publication, Ensuring Proper Use of Electronic Health Record Features and Capabilities: A Decision Table, they share their trepidation with copying text:
This can affect the quality of care and can cause improper payments due to:
- False impression of services provided to the patient.
- Coding from old or outdated information that may lead to “upcoding.”
To better illustrate the hazards related to coding and billing, Ventra has compiled examples of copied text that has led to upcoding:
- Complexity of problems addressed (COPA) was overstated:
- The history of the present illness was copied forward into subsequent visits with no interval updates. On day four of the stay, the patient had improved greatly but not according to the unedited history. This led the coder to believe that at the time of the visit, the illness was more severe than it was.
- The assessment included more conditions than what were addressed on the date of service.
- Data was falsely inflated:
- The section “Data Reviewed” included test results from previous days that were already reviewed and credited for coding.
- The plan brought forward orders for diagnostics that were already completed and already credited for coding.
- Risks were misrepresented: The plan read as if new (treatment) orders were placed and procedures were scheduled, yet they were already done and already credited for coding.
To reduce coding errors that could result in overpayment, CMS has made suggestions for safeguarding the integrity of documentation:
- Create a policy on copy and paste and weigh efficiency against the potential for inaccurate, fraudulent, or unmanageable documentation.
- Set a policy requiring the provider to modify copied information to be patient-specific and related to the current visit.
- Set policy controlling and limiting the use of the copy and paste function.
- Include proper notation and clear attribution of copied information.
- Set policy making clear the use of cut and paste, as it changes the original source material.
- Monitor and audit copy and paste usage in the audit log. If possible, enable the EHR system to record the method of each data entry (for example, copy and paste or direct text entry).
Ventra has personally witnessed the challenges physicians have faced under audit. We have found it to be a long and arduous road defending and appealing claims, as we have spent hours poring through records, trying to determine what was related to the visit under review and what could be used for coding. No practice wants to find themselves at the receiving end of a CMS audit. For this reason, our Provider Education team of experts recommends:
- Using copy-and-paste features sparingly.
- Indicating the information is copied so that it can be easily recognized as such and not used repeatedly for coding. This can be accomplished by dating the cloned text.
- Encouraging providers to document an interval history for all subsequent visits.
- Creating a new assessment and plan for each encounter.
What’s Next and How Ventra Health Can Help
Ventra Health takes compliance very seriously. Our Provider Education team has launched this Compliance Blog Series to help you navigate the complexities of compliance and coding changes. In case you missed it, check out our other posts in the series.
→ Learn More About Provider EducationGet your Strategy Sheet for 2024 MIPS Success
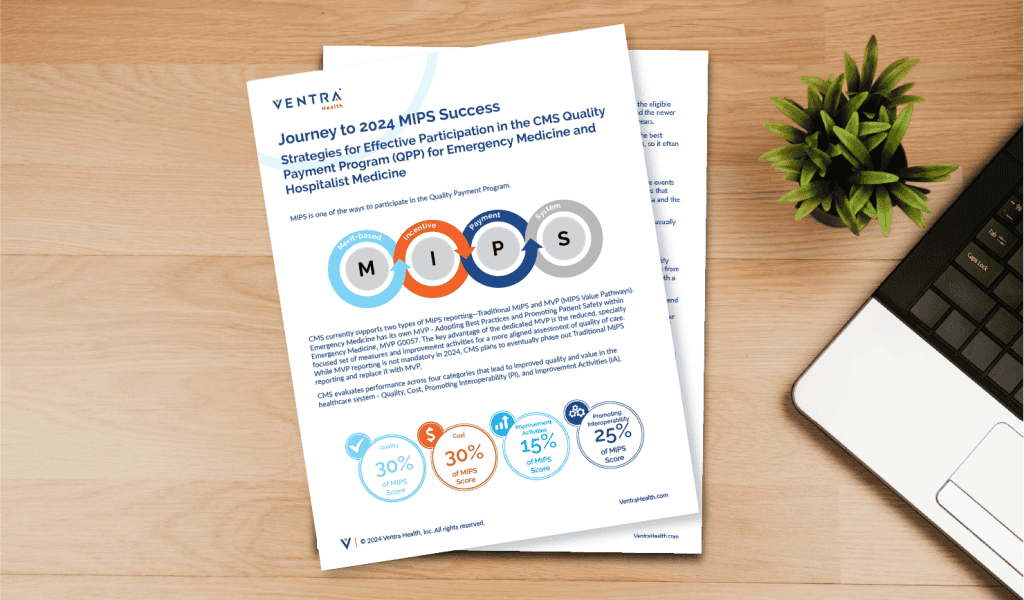
Journey to 2024 MIPS Success: Strategies for Effective Participation in the CMS Quality Payment Program (QPP)
The Merit-based Incentive Payment System (MIPS) is one way to participate in CMS’ Quality Payment Program. CMS currently supports two types of MIPS reporting—Traditional MIPS and MVP (MIPS Value Pathways). If you’re not sure where to start, check out these strategies to achieve MIPS success in 2024.
→ Download NowDisclaimer: This document is for educational purposes only and was created based on information known at the time of its release. Though Ventra Health has made every attempt to produce accurate and up-to-date information, the payer’s expectations and interpretations may change or differ from those of Ventra, and Ventra therefore makes no guarantee and shall have no liability for the actual results or outcomes. Providers bear the responsibility of the overall quality, content, and medical necessity of their documentation. Ventra Health does not provide legal advice, and neither this document nor any other discussions with Ventra should be considered legal advice. Please seek counsel from your own legal counsel for any legal advice.


